
Nasal septal deviation is one of the most common anatomical findings in otolaryngology practice. It affects a large portion of patients who come in with chronic nasal obstruction, recurrent sinusitis, and sleep disordered breathing. When conservative management does not provide meaningful relief, septoplasty becomes the procedure of choice. Its success depends heavily on the quality and completeness of the septoplasty instrument set used during the operation. Having the right instruments, properly arranged and well maintained, has a direct effect on operative efficiency, precision in tissue handling, and the risk of complications during surgery.
This guide is written for ENT surgeons, surgical residents rotating through rhinology, OR nurses responsible for instrument setup, and hospital procurement teams evaluating surgical instrumentation for their rhinology program. It covers everything that goes into a well designed septoplasty instrument set, starting with its defining characteristics and clinical rationale, moving through a structured instrument list, and ending with practical guidance on surgical use and maintenance.
What Is a Septoplasty Instrument Set?
A septoplasty instrument set is a curated collection of surgical instruments designed specifically to support the correction of nasal septal deformities. Unlike general ENT trays, which include instruments suited to a range of procedures, a dedicated septoplasty set is built around the anatomical demands of the nasal septum, a midline structure made up of both cartilaginous and bony elements that requires precise dissection, controlled resection, and careful reconstruction.
The instruments in a complete septoplasty set are manufactured from high-grade surgical stainless steel, which resists corrosion during repeated sterilization cycles while maintaining the structural rigidity required for controlled force application. Premium sets use a satin or matte finish to minimize intraoperative light glare, a practical detail that improves visualization in a confined surgical field. The instruments are precision machined to maintain consistent tolerances across the set, so forceps close squarely, scissors cut cleanly, and elevators engage tissue without slipping.
A septoplasty instrument set supports the core operative sequence: mucoperichondrial and mucoperiosteal elevation, cartilage scoring and resection, bony spur removal, and final mucosal closure. Sets designed for comprehensive rhinology programs may also accommodate concurrent procedures such as inferior turbinate reduction or functional endoscopic sinus surgery when paired with the appropriate supplemental instruments.
Why a Dedicated Septoplasty Instrument Set Matters Clinically
The nasal septum presents a unique surgical environment. The mucoperichondrium and mucoperiosteum are thin, adherent membranes that need to be elevated cleanly from the underlying cartilage and bone without perforation. A tear in either mucosal layer, particularly a bilateral perforation, can result in a persistent septal perforation, one of the most challenging complications to manage in rhinologic surgery. This anatomical reality calls for instruments designed with the right geometry, edge quality, and tactile feedback so the surgeon can work confidently in a tight space.
A dedicated set matters for three interconnected reasons. The first is precision. Instruments built specifically for septoplasty have blade profiles, shaft lengths, and handle ergonomics calibrated for work within the nasal cavity, where a poorly angled elevator or an oversized speculum can compromise both visibility and tissue control. The second is workflow. When a set is standardized and complete, the scrub technician can anticipate instrument handoffs, which reduces operative time and cuts down on the distraction that comes from improvised substitutions mid case. The third is patient safety. Instruments correctly matched to the tissue type and surgical step reduce the force required for each maneuver, which directly lowers the risk of accidental mucosal perforation, injury to the nasal spine, or excessive bleeding from disrupted vessels along the bony cartilaginous junction.
From a procurement standpoint, investing in a comprehensive, high quality septoplasty set also protects the facility against the longer term costs of instrument failure, frequent instrument borrowing from adjacent trays, and the delays that come with incomplete setups.
Clinical Indications
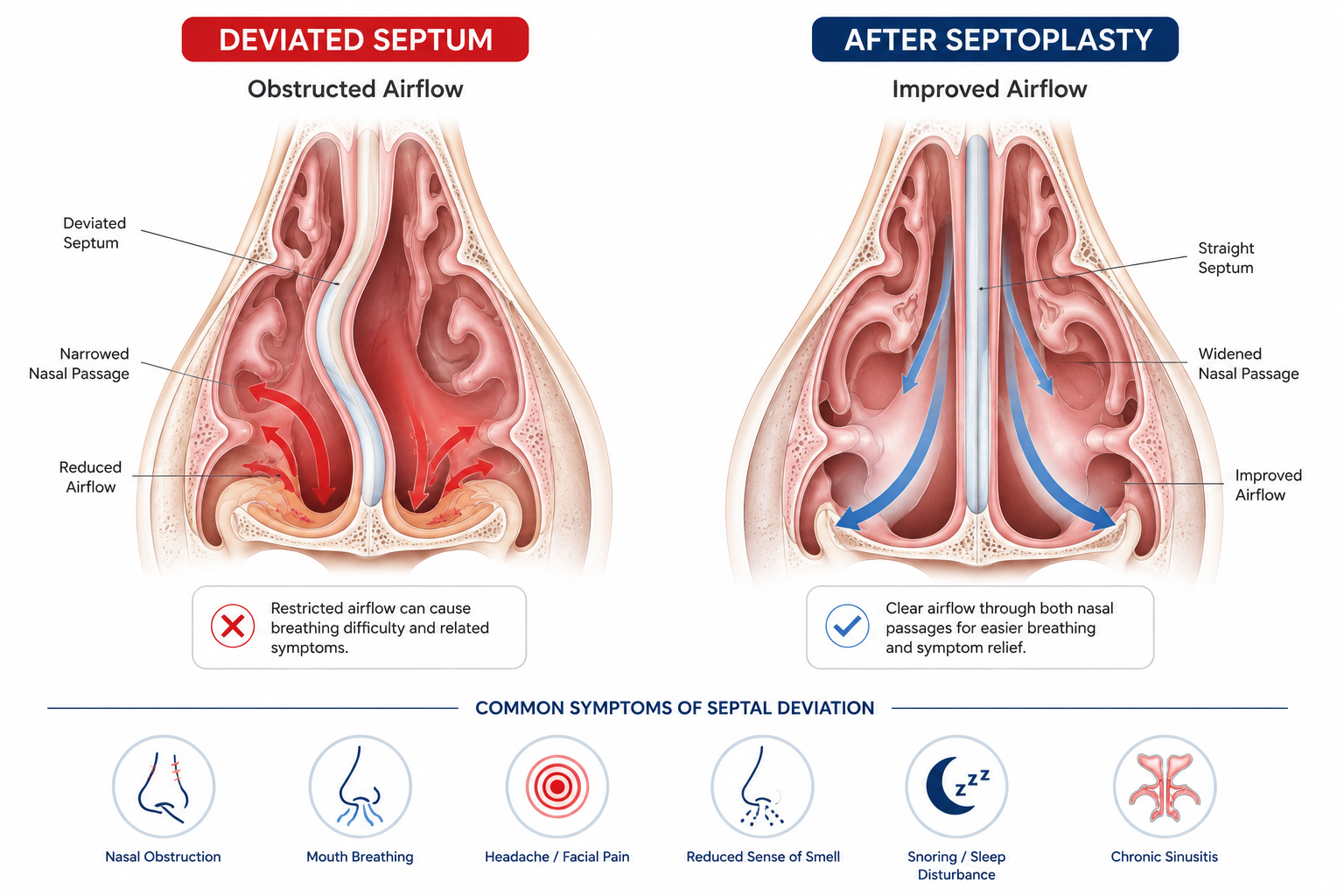
The most common reason for septoplasty is symptomatic nasal obstruction caused by septal deviation that has not responded to medical management, including topical corticosteroids and antihistamines. Patients typically report unilateral or bilateral nasal blockage, reduced airflow, and related symptoms such as mouth breathing, chronic headache, or hyposmia. The decision to proceed surgically is based on endoscopic confirmation of an anatomically significant deviation and how well it correlates with the patient’s reported symptoms.
A second major indication is recurrent or chronic rhinosinusitis, where septal deviation contributes to impaired mucociliary drainage or narrows the middle meatus to the point where medical therapy cannot adequately reach the sinus ostia. In these patients, septoplasty is often performed alongside functional endoscopic sinus surgery to address both the obstructing anatomy and the underlying sinus disease at the same time.
Septoplasty is also indicated in patients with obstructive sleep apnea or snoring when nasal obstruction is identified as a contributing factor, particularly when mandibular advancement devices or continuous positive airway pressure tolerance is compromised by poor nasal patency. Epistaxis management is a less common but well recognized indication. A prominent septal spur or a deviated caudal septum with mucosal thinning can cause recurrent anterior bleeding that is best addressed surgically.
Reconstructive septoplasty is performed following nasal trauma with associated septal fracture or dislocation, and it may also be indicated in patients undergoing rhinoplasty who need structural cartilage grafting from the septum for dorsal or tip support. In these cases, the septoplasty instrument set must accommodate a broader scope of dissection and cartilage harvest.
History and Pioneers of Septal Surgery
The surgical correction of nasal septal deformity has evolved over more than a century of rhinologic practice, shaped by a succession of surgeons who built on each other’s work and responded to the complications they observed in earlier techniques.
The late nineteenth century saw the first attempts at correcting septal deviation through forcible fracture and splinting, and later through more aggressive resection approaches. Ephraim Fletcher Ingals contributed to this early period of nasal surgery, but the foundational advance came in the early twentieth century when Otto Tiger Freer of the United States in 1902 and Gustav Killian of Germany in 1904 each independently described the submucous resection operation. Their shared principle was that the mucoperichondrium should be elevated intact from the underlying cartilage and bone before any resection was attempted. This elevation-first approach established the anatomical logic that still defines septoplasty today, and it is why many instruments in current use, including the Freer elevator and the Killian speculum, carry their names.
The submucous resection technique, while a major improvement over what came before it, involved removing substantial amounts of septal cartilage and bone. Over time, long-term follow-up of these patients revealed a recognizable pattern of late complications, including dorsal saddling, columellar retraction, and alar widening, all resulting from the loss of structural support that the resected cartilage had provided. This pushed the field toward a more conservative philosophy.
In 1929, Metzenbaum described the swinging door technique for addressing caudal septal dislocation, one of the areas where submucous resection was least effective. Peer followed in 1937, advocating removal of the displaced caudal septum, reshaping it outside the nose, and replacing it in the midline as a graft. These contributions introduced the concept of cartilage repositioning rather than simple removal.
Cottle’s work, formalized with the introduction of the hemitransfixion incision in 1947 and his maxilla-premaxilla approach presented in 1958, marked the clearest philosophical break from aggressive resection. Cottle and his colleagues emphasized conservative resection, cartilage preservation, and reconstruction of the septal framework rather than its removal. This philosophy directly influenced instrument design in the decades that followed, shifting the preference toward tools built for controlled, selective tissue management rather than broad excision. The Cottle elevator, still a standard component of modern septoplasty sets, reflects this approach in its geometry and edge profile.
Understanding this history matters clinically because every significant design choice in a modern septoplasty instrument set traces back to a lesson learned from an earlier complication. The geometry of an elevator blade, the controlled width of an osteotome, the angled profile of nasal scissors, none of these details are arbitrary. They are the accumulated result of a field that spent decades refining what happens when the wrong tool is used at the wrong moment in this surgery.
Septoplasty Instruments: Complete Set with Names and Functions
| Category | Common Instruments Included | Primary Clinical Use |
|---|---|---|
| Specula and Retractors | Killian Nasal Speculum (small, medium, large), Vienna Nasal Speculum, Cottle Columellar Retractor | Dilate the nasal vestibule and maintain visualization throughout the operative field. The Killian speculum is the workhorse retractor for septoplasty, providing exposure of the caudal septum and nasal floor. |
| Elevators and Dissectors | Freer Septum Elevator (double-ended), Cottle Elevator, Jansen-Middleton Elevator, McKenty Elevator | Elevate the mucoperichondrium and mucoperiosteum from the cartilaginous and bony septum. The Freer elevator’s sharp and blunt ends allow transition between initial incision-site entry and broader flap elevation. |
| Knives and Scalpels | No. 15 Blade Handle (Bard-Parker), Cottle Nasal Knife, Ballenger Swivel Knife | Make the hemitransfixion or Killian incision at the caudal septum. The Ballenger swivel knife allows the surgeon to score and section cartilage at varying angles without excessive manipulation of surrounding tissue. |
| Scissors | Metzenbaum Scissors (curved, small), Goldman-Fox Scissors, Mayo Scissors (straight), Iris Scissors | Sharply divide mucosal attachments, trim redundant mucosa, and cut sutures during closure. Goldman-Fox scissors are particularly suited to confined nasal spaces given their angled, narrow blade profile. |
| Forceps and Tissue Graspers | Jansen-Middleton Septum Forceps, Takahashi Nasal Forceps, Bayonet Forceps, Adson Tissue Forceps (1×2 teeth), Gerald Forceps | Grasp, stabilize, and remove cartilaginous and bony septal fragments. The Jansen-Middleton forceps is designed specifically for biting through and extracting deviated septal cartilage, while bayonet forceps allow instrument passage alongside other tools without obstructing the surgeon’s sightline. |
| Chisels, Osteotomes, and Mallets | Cottle Osteotome (4mm, 6mm), Rowe Disimpaction Forceps, Surgical Mallet | Release and mobilize bony septal elements, particularly the perpendicular plate of the ethmoid and the vomer. Essential for cases involving high septal deviations or bony spurs at the bony-cartilaginous junction. |
| Rongeurs and Punches | Jansen-Middleton Rongeur, Hartmann Nasal Punch, Blakesley Nasal Forceps (straight and angled), Kerrison Rongeur | Incrementally remove bony projections and reduce septal spurs with controlled bites. The Blakesley forceps provides through-cutting action that minimizes tissue tearing compared with avulsion-based removal. |
| Suction and Irrigation | Frazier Suction Tip (5 Fr, 7 Fr), Baron Suction Tip, Yankauer Suction | Maintain a clear operative field by continuously clearing blood and irrigation fluid. The Frazier tip’s narrow barrel is well suited to the confined nasal space and can be directed precisely without obscuring the surgeon’s view. |
| Needle Holders and Suturing | Crile-Wood Needle Holder, Webster Needle Holder (fine), Halsted Mosquito Forceps | Facilitate mucosal closure with absorbable suture. The Webster needle holder’s slender profile is preferred for suturing within the nasal vestibule and at the columellar incision site. |
| Packing and Splinting Instruments | Nasal Packing Forceps (Graney or equivalent), Bayonet Dressing Forceps | Place absorbable or non-absorbable nasal packing at the close of the procedure, or position silicone septal splints when stabilization of the reconstructed septum is indicated. |
Step-by-Step Clinical Use of the Septoplasty Instrument Set
The operation starts with positioning the patient, head slightly raised with the neck gently extended to line up the nasal axis. The surgeon then injects a vasoconstrictor, usually 1% lidocaine with 1:100,000 epinephrine, into the caudal septum and nasal floor on both sides. Next comes the Killian nasal speculum, which opens up the nasal vestibule and exposes the caudal septum. The size is picked based on the patient’s nose, and this speculum stays in use for most of the surgery.
Using a No. 15 blade on a Bard Parker handle, the surgeon makes a hemitransfixion incision just in front of the septal cartilage, staying in the mucosal layer where the columella meets the caudal septum. Some surgeons prefer a Killian incision instead, placed a bit further back depending on where the deviation is. Once the incision is made, the Freer elevator goes in with its sharp end to find the subperichondrial plane. Getting into the right plane matters here. The elevation should move easily, and the surgeon feels through the handle whether they are in the correct layer.
After the flap is lifted on one side, the Cottle or McKenty elevator carries it back and up over the cartilage bone junction, moving into the mucoperiosteal plane over the perpendicular plate and vomer. The same steps are repeated on the other side, working through the tunnel made by the first incision. With both flaps up, the deviated parts of the septum are now visible and accessible.
To correct the cartilage, the surgeon uses the Ballenger swivel knife or a straight nasal knife to score and cut the deviated cartilage. The Jansen Middleton septum forceps then removes the cut piece, or repositions it if a more conservative approach is being used. For bone deviations, the Cottle osteotome is tapped in with a mallet to free the perpendicular plate or vomer, and the Jansen Middleton or Kerrison rongeur trims down bony projections bit by bit until the septum sits straight. The assistant keeps suctioning with the Frazier tip throughout to keep the view clear.
Once the main correction is done, the flaps are laid back in place and checked for tears. Any small tears are stitched closed with absorbable suture using the Webster needle holder and fine Gerald or Adson forceps. The original incision is then closed the same way. If splints are needed to hold the septum straight while it heals, silicone splints go in, held with bayonet dressing forceps and nasal packing forceps.
Safety Considerations in Septoplasty Instrumentation
The nasal septum sits close to several important structures, and the instruments chosen for each step directly affect how much margin for error the surgeon has. Toward the top, aggressive dissection or a poorly directed osteotome can damage the cribriform plate, risking a cerebrospinal fluid leak. This is uncommon but serious. The Cottle osteotome is built with a controlled cutting width so the surgeon can work the bone precisely while keeping the depth and angle of each stroke in check.
Septal perforation is the most common significant complication of septoplasty, and it is closely tied to how well the mucosa is elevated. An elevator with a dull or worn edge needs more force to do its job, and that extra force raises the chance of tearing the mucoperichondrium. This is why keeping instruments in good condition, sharpening elevator edges regularly and replacing anything showing wear, is not just about efficiency. It is about patient safety. A well maintained Freer elevator that moves smoothly through the subperichondrial plane behaves very differently from one that catches and tears tissue.
Good hemostasis tools, particularly fine mosquito forceps and proper suction, lower the risk of a postoperative hematoma, which can turn into a septal abscess if it is not caught and drained early. The Frazier suction tip’s thumb controlled vent lets the surgeon adjust suction strength on the spot, which helps avoid injuring delicate mucosal edges near a perforation site or during closure.
Sterilization, Maintenance, and Set Standardization

Every instrument in a septoplasty set should hold up to steam autoclave sterilization, typically 134 degrees Celsius for three to four minutes in prevacuum cycles, or 121 degrees Celsius for thirty minutes in gravity displacement cycles. Before sterilization, instruments need to be cleaned ultrasonically or by hand with warm water and enzymatic detergent to clear out organic debris from box joints, serrated jaws, and any surfaces that touch tissue. Instruments with box joints, such as the Killian speculum, Jansen Middleton forceps, and rongeurs, need extra attention so debris does not build up in the joint and affect how smoothly they open and close during surgery.
Checking cutting edges regularly is important too. Elevator blades, nasal knives, and scissors should be inspected under magnification at set intervals to spot dullness, chipping, or corrosion. Any instrument showing signs of wear, including cracked handles, sprung forceps jaws, or loose box joints, should be pulled from use right away. Borrowing instruments from other trays to fill gaps in a depleted septoplasty set is a common cause of slowdowns during surgery, and it can usually be avoided with disciplined set management and timely reordering.
Standardizing the septoplasty instrument set across an ENT program brings real operational benefits. When the whole surgical team works with the same instruments arranged the same way, scrub technicians can anticipate handoffs reliably, which cuts down on the time surgeons spend waiting and reduces communication errors during critical moments of dissection. Standardization also makes instrument tracking easier, shortens sterilization turnaround time, and simplifies procurement by cutting down on the number of unique SKUs central supply has to manage.
Conclusion
A well configured septoplasty instrument set is not a side consideration in rhinologic surgery. It is a clinical requirement. From the precision of the Freer elevator’s edge during mucoperichondrial elevation, to the controlled bite of the Jansen Middleton rongeur during bony spur reduction, every instrument in the set plays a part in helping the surgeon reach the procedure’s anatomical goals while keeping the risk of complications low. The case for investing in a comprehensive, high quality set is strong on both clinical and procurement grounds. Better instruments support better outcomes, smoother operative workflows, and lower total cost of care over time.
For ENT programs building or refreshing their rhinology instrument inventory, the septoplasty instrument set is a foundational investment. As surgical techniques keep evolving, with more endoscopic approaches and image guided navigation coming into use, the underlying instrument set remains the constant that operative excellence is built on. Carnegie Surgical LLC is committed to providing ENT surgeons and hospital systems with septoplasty instrument sets engineered to meet the demands of modern rhinologic practice.
References
- Setzen G, Ferguson BJ, Han JK, et al. Clinical consensus statement: Appropriate use of computed tomography for paranasal sinus disease. Otolaryngology–Head and Neck Surgery. 2012;147(5):808–816. https://pubmed.ncbi.nlm.nih.gov/22935902/
- Fokkens WJ, Lund VJ, Hopkins C, et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinology. 2020;58(Suppl S29):1–464. https://pubmed.ncbi.nlm.nih.gov/32077450/
- Bloom JD, Kaplan SE, Bleier BS, Goldstein SA. Septoplasty complications: avoidance and management. Otolaryngologic Clinics of North America. 2009;42(3):463–481. https://pubmed.ncbi.nlm.nih.gov/19486879/
- Fettman N, Sanford T, Sindwani R. Surgical management of the deviated septum: techniques in septoplasty. Otolaryngologic Clinics of North America. 2009;42(2):241–252. https://pubmed.ncbi.nlm.nih.gov/19328888/
- Bhattacharyya N. Ambulatory sinus and nasal surgery in the United States: demographics and perioperative outcomes. Laryngoscope. 2010;120(3):635–638. https://pubmed.ncbi.nlm.nih.gov/20025027/
- Most SP. Anterior septal reconstruction: outcomes after a modified extracorporeal septoplasty technique. Archives of Facial Plastic Surgery. 2006;8(3):202–207. https://pubmed.ncbi.nlm.nih.gov/16769892/
- Roblin DG, Eccles R. What, if any, is the value of septal surgery? Clinical Otolaryngology. 2002;27(2):77–80. https://pubmed.ncbi.nlm.nih.gov/11994101/
- Flint PW, Haughey BH, Lund VJ, et al. Cummings Otolaryngology: Head and Neck Surgery. 7th ed. Philadelphia: Elsevier; 2021. Chapter 43: Surgery of the Nasal Septum.